Does your child’s dry, itchy rash mean they are destined for a lifetime of asthma and food allergies? For decades, doctors believed in a strict timeline called the atopic march, which is the sequential progression of allergic diseases starting with eczema in infancy and evolving into food allergies, rhinitis, and asthma. The idea was simple: if you have eczema first, the other conditions will inevitably follow. But recent science tells us this isn't quite true anymore. In fact, only about 3.1% of children follow that exact linear path. So, what is actually happening when a baby develops eczema, and how can you protect their health without falling for old myths?
The Myth of the Inevitable Progression
We need to clear up a major misconception right away. The traditional view of the atopic march suggested a one-way street from skin issues to breathing problems. However, modern research has shifted toward a concept called atopic multimorbidity, which refers to the coexistence of multiple allergic conditions rather than a strict sequential order. This means these conditions often happen together or overlap, rather than following a rigid script.
Consider the numbers. Approximately 17-24% of children worldwide develop atopic dermatitis (commonly known as eczema). While this is common, it does not guarantee future allergies. Studies show that only about 25% of children with eczema go on to develop asthma. That leaves 75% who do not. Why did the old model persist? It helped identify high-risk groups early. But relying on it now can cause unnecessary panic. Instead of assuming every case of eczema leads to asthma, we look at severity. Severe eczema increases the risk of asthma by over 60% compared to mild cases. This distinction is crucial for parents and clinicians alike.
The Broken Door: How Skin Barriers Work
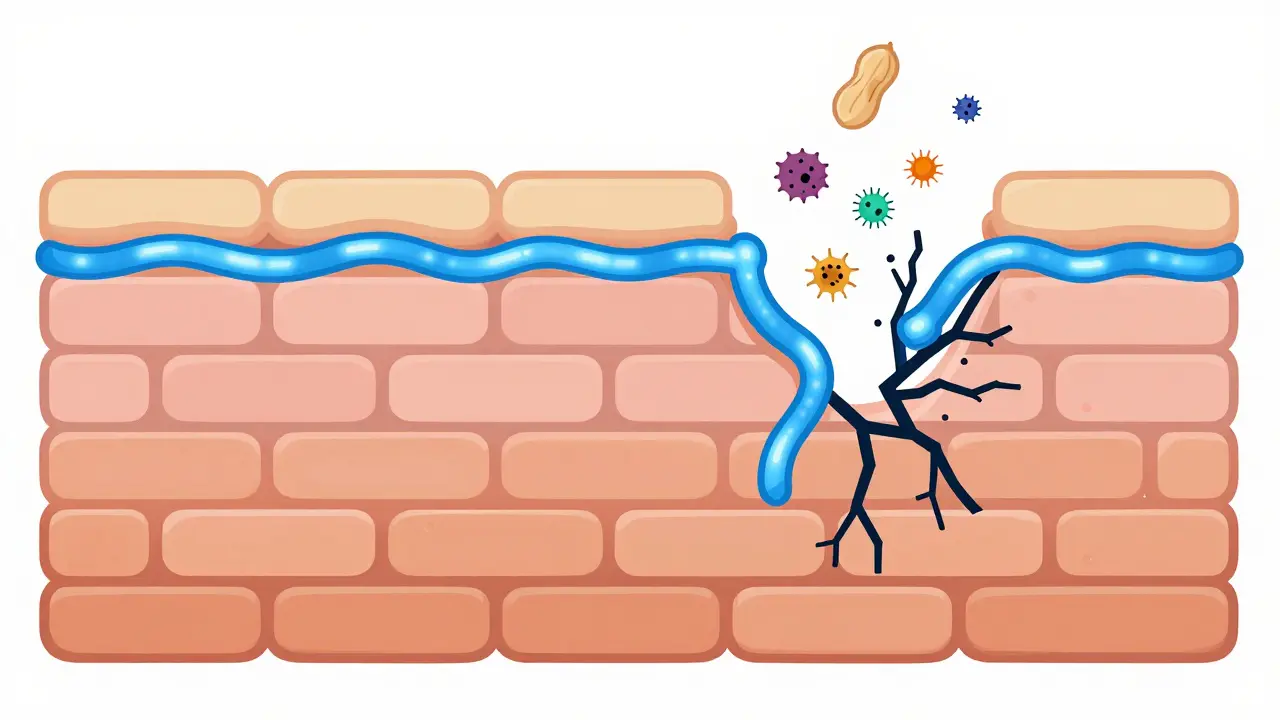
To understand why allergies develop, you have to look at the skin itself. Think of healthy skin as a brick wall. The bricks are skin cells, and the mortar holding them together is a protein called filaggrin, which is a structural protein in the epidermis that maintains the skin barrier and prevents allergen penetration. When this mortar is weak or missing, the wall crumbles. Allergens like peanut proteins, dust mites, or pet dander slip through the cracks.
This isn't just a theory. Genetic studies have identified loss-of-function mutations in the filaggrin gene as a primary driver of this process. About 10-20% of people with severe eczema carry these mutations. But here is the twist: having the mutation alone doesn't automatically cause food allergies. It requires the presence of active eczema. When the skin is inflamed and cracked, immune cells encounter these foreign substances for the first time. Instead of ignoring them, the immune system sounds the alarm. This is sensitization. The body starts producing IgE antibodies against harmless things like eggs or milk because they entered through the broken skin, not the mouth.
Dual Allergen Exposure: Skin vs. Gut
This brings us to the dual-allergen exposure hypothesis, which posits that allergen exposure through defective skin causes sensitization, while oral exposure promotes tolerance. It sounds counterintuitive, but it makes sense when you look at biology. Your gut is designed to handle food. It has mechanisms to break down proteins and signal safety. Your skin is not. It is designed to keep things out. When food proteins hit damaged skin, the immune system treats them as invaders.
The LEAP study (Learning Early About Peanut Allergy) provided massive proof for this. They found that introducing peanut protein orally to high-risk infants reduced peanut allergy development by 86%. Meanwhile, avoiding peanuts entirely did nothing to prevent allergies and might have made them worse by allowing skin exposure to dominate. This shift in understanding changed global guidelines. We no longer tell parents to avoid allergens until age three. We encourage early, safe oral introduction while simultaneously fixing the skin barrier.
Beyond Genetics: The Role of Microbiome and Environment
Genetics load the gun, but environment pulls the trigger. Recent research highlights the importance of the gut microbiome in regulating immune responses and influencing the development of allergic sensitization. Infants who develop multi-sensitized atopy often have gut bacteria with reduced genetic potential for butyrate fermentation. Butyrate is a short-chain fatty acid that helps maintain gut integrity and calm inflammation. Without enough of it, the immune system stays on high alert.
Environmental factors also play a huge role. Urban living, lack of microbial diversity, and excessive hygiene can alter both skin and gut bacteria. Dr. Supinda Bunyavanich notes that neonatal gut microbiota associates strongly with childhood T-cell differentiation. If the immune system learns to differentiate poorly early on, it may attack harmless antigens later. This suggests that interventions targeting the microbiome-through diet, probiotics, or even environmental exposure-could potentially alter disease trajectories before symptoms appear.

Skin Barrier Care: The First Line of Defense
If the skin barrier is the key entry point for allergens, then repairing it is the most logical intervention. This is where proactive skincare comes in. It’s not just about treating flare-ups; it’s about preventing them. Emollients (moisturizers) help restore the lipid layer of the skin, filling in those microscopic cracks.
The PreventADALL trial is currently investigating whether early emollient therapy can prevent atopic dermatitis and subsequent allergic conditions. Preliminary results are promising, showing a 20-30% reduction in eczema incidence among infants who received daily moisturizing. The strategy is simple: apply thick, fragrance-free creams immediately after bathing to lock in moisture. Look for ingredients like ceramides, which mimic the natural lipids in the skin. Avoid harsh soaps and hot water, which strip away natural oils. By keeping the skin intact, you reduce the chance of allergens penetrating and triggering an immune response.
| Factor | Impact on Progression | Intervention Strategy |
|---|---|---|
| Filaggrin Mutation | High risk of barrier defect | Aggressive moisturizing routine |
| Mild Eczema | Low risk of asthma (<20%) | Standard barrier repair |
| Severe Eczema | High risk of asthma (>60%) | Medical management + barrier care |
| Early Oral Allergen Intro | Reduces food allergy risk by 86% | Introduce peanuts/eggs early (if safe) |
Clinical Implications: Precision Over Panic
So, what should you do if your child has eczema? First, don’t panic. Remember that only a small fraction progress to full-blown atopic multimorbidity. Second, focus on severity. If the eczema is mild and well-controlled, the risk of developing asthma remains low. If it is severe, persistent, and difficult to treat, consult an allergist. They can assess for specific risk factors like filaggrin mutations or family history of asthma.
Third, prioritize skin barrier care. Make moisturizing a non-negotiable part of your daily routine. Fourth, consider early oral introduction of common allergens under medical guidance. Don’t avoid foods unless there is a diagnosed allergy. Finally, be aware of environmental triggers. Dust mites, pet dander, and pollen can exacerbate skin inflammation. Reducing exposure to these irritants can help keep the skin calm and closed.
The goal is not to predict the future but to influence it. By understanding the complex interplay between genetics, skin barrier function, and immune development, we can take proactive steps. We move from a passive acceptance of the "march" to an active effort to "arrest" it. This precision approach empowers parents and clinicians to make informed decisions based on individual risk profiles rather than broad generalizations.
What is the atopic march?
The atopic march is a historical term describing the progression of allergic diseases, typically starting with eczema in infancy and moving to food allergies, allergic rhinitis, and asthma. Modern research suggests this linear model is rare, with only 3.1% of children following this exact path. Most cases involve overlapping conditions known as atopic multimorbidity.
Does eczema always lead to asthma?
No. Only about 25% of children with eczema develop asthma. The risk is significantly higher for those with severe, uncontrolled eczema. Mild eczema that is well-managed carries a much lower risk of progressing to respiratory allergies.
How does filaggrin affect allergies?
Filaggrin is a protein that acts as mortar in the skin's barrier. Mutations in the filaggrin gene weaken this barrier, allowing allergens to penetrate the skin and trigger immune sensitization. This is a key genetic link between eczema and subsequent food or airway allergies.
Should I introduce peanuts early to my baby?
Yes, current guidelines recommend early oral introduction of peanut protein (around 4-6 months) for infants, especially those with eczema, to promote tolerance. The LEAP study showed this reduces peanut allergy risk by 86%. Always consult your pediatrician before introducing potential allergens.
Can moisturizer prevent eczema?
Daily use of emollients can strengthen the skin barrier and may reduce the incidence of eczema by 20-30%, according to trials like PreventADALL. While it may not eliminate genetic risks, maintaining a healthy barrier reduces allergen penetration and inflammation.